CASE REPORT / OLGU SUNUMU
Doi: 10.5798/diclemedj.0921.2012.01.0106
Multiple myeloma masquerading as a pulmonary mass: A rare presentation
Akciğerde bir kitle olarak maskelenen multiple
miyeloma: Nadir bir ortaya çıkış
Sunita Singh, Promil Jain, Mansi Kala, Rajeev Sen
Department of Pathology, Pt BDS PGIMS, Rohtak, India
Yazışma Adresi /Correspondence: Dr. Promil Jain, Pathology Department, 157, L-1,
Model town, Rohtak, Haryana-India
Email: jainpromil@gmail.com
Geliş Tarihi / Received: 05.08.2011, Kabul Tarihi /
Accepted: 11.01.2012
ABSTRACT
Multiple myeloma represents
malignant disorder of plasma cells. Tumour extension is primarily seen within
the bone and bone marrow, despite widespread distribution of plasma cells in
the body. Metastatic deposits outside bone marrow (extramedullary) are uncommon
even in advanced multiple myeloma. Involvement of pulmonary parenchyma by
myeloma cells either as plasmacytoma or as a pulmonary infiltrate is rare and
is related to aggressive terminal phase of the disease. We are reporting a case
of multiple myeloma with a pulmonary parenchymal mass as the initial presenting
manifestation.
Key words: Pulmonary, multiple myeloma,
extramedullary plasmacytoma (EMP).
ÖZET
Multiple
miyeloma plazma hücrelerinin malign hastalığıdır. Plazma hücreleri vücutta
yaygın olarak bulunmakla birlikte, tümör genellikle kemik ve kimik iliği içine
yayılır. İlerlemiş vakalarda bile ilik dışına metasazla yayılımı nadirdir.
Akciğer parankiminin miyelom hücrelerei tarafından gerek plazmositoma olarak
gerekse akciğer metastazı olarak tutulumu nadirdir ve hastalığın agresif terminal dönemi ile ilgilidir. Burada ilk olarak
akciğer parankim kitlesi olarak belirti veren bir multiple miyeloma olgusunu
sunuyoruz.
Anahtar kelimeler: Akciğer,
multiple miyelom, ekstrameduller plazmositom.
INTRODUCTION
Multiple myeloma is a neoplasm
of B cell lineage characterised by excessive proliferation of abnormal plasma
cells involving primarily the bone marrow. These malignant plasma cells secrete
an abnormal immunoglobulin causing a monoclonal gammopathy.1 The disease process mainly involves the axial skeleton. The
occurrence of extramedullary disease is uncommon in multiple myeloma.2
Reported extramedullary sites include liver, spleen and lymph nodes.3
Lung parenchymal involvement in multiple myeloma is extremely rare.4
The prognosis of patient with pulmonary involvement is poor and is more
commonly associated with aggressive terminal phase of myeloma.3 Here
we are reporting an interesting case of multiple myeloma masquerading as a
pulmonary mass with thoracic extension involving D4-D8 vertebrae and adjacent
ribs.
CASE
A 50 years old male presented
to the department of Chest and Tuberculosis at Post Graduate Institute of
Medical Sciences, Rohtak, India with a vague complaint of chest pain, cough and
mild breathlessness of 6 months duration. The pain was moderate in intensity
and constant. He was a non-smoker and non-alcoholic. There was no history of
fever or preceding trauma. Chest radiograph showed a peripheral shadow
involving right upper and middle zone and extending beyond the thoracic cage.
Physical examination of the patient revealed no significant abnormality except
mild pallor. Routine investigations revealed Hb-9.6 g/dl, TLC-9800/cm3
with neutrophils-70%, lymphocytes-23%, eosinophils-2%, monocytes-5%. ESR was
A subsequent skull radiograph revealed multiple
punched out lytic lesions (Fig. 2) Contrast tomography (CT) examination of
chest revealed large peripheral lung mass with smooth margins in lateral
segment of right middle lobe showing homogenous contrast enhancement. The mass
was extending in the costovertebral space of D-4 to D-8 vertebrae alongwith
erosion of the adjacent vertebra and ribs (Fig. 3).
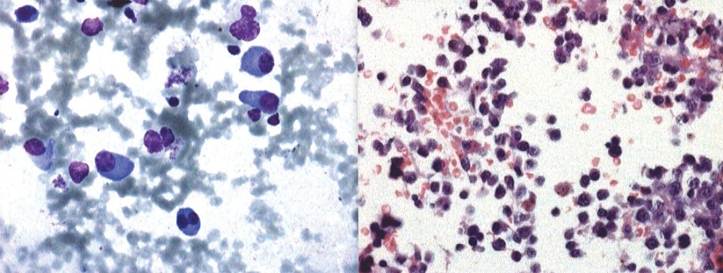
Figure 1 a&b. FNAC and biopsy lung: Photomicrograph revealing
plasma cell infiltrate (Giemsa 400X, H & E 400X)

Figure 2. X-ray skull: showing multiple punched out lytic
lesions
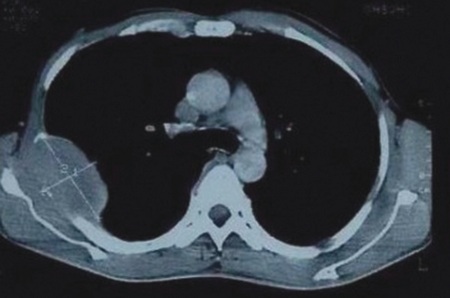
Figure 3. CT scan showing mass in lung extending in thoracic
cage and lytic lesion in D-4 to D-8 Vertebra
Bone marrow aspiration revealed about 10% plasma
cells. Serum protein electrophoresis revealed normal total serum proteins
(7.8gm/dl), mildly raised gamma globulin -1.84g/dl, (normal 0.6-1.6g/dl) and
normal serum albumin, alpha 1, alpha 2 and beta globulin. Bence Jones
proteinuria was absent. Immunofixation showed A/G -1.42, serum IgG -17.1g/dl
(normal 6.94-16.2 g/dl), serum IgA-2.38g//l, serum IgM -0.82 g/l, serum free
Kappa (light chain) 2.50mg/dl (normal 0.33-1.94 mg/dl), serum free lambda
(light chain) 1.03mg/dl, serum free kappa/lamda ratio-2.42 (normal 0.26-1.65).
It showed monoclonal band in serum protein electrophoresis lane, corresponding
to monoclonal band seen in IgG and Kappa lanes suggestive of IgG kappa
monoclonal gammopathy. A final diagnosis of multiple myeloma with dissemination
in pulmonary parenchyma and adjoining soft tissues was made.
DISCUSSION
Multiple myeloma is a
haematological malignancy characterised by malignant clonal proliferation of
plasma cells in the bone marrow. It is associated with serum monoclonal
protein, skeletal destruction with osteolytic lesions, pathological fractures,
bone pains, hypercalcemia, renal failure, and anemia. The disease spans a
spectrum from localised, smoldering or indolent to aggressive, disseminated
forms with plasma cell infiltration of various organs, plasma cell leukemia,
and disorders due to deposition of abnormal immunoglobin chains in tissues. Generalised
bone marrow involvement in multiple myeloma is typically present.5
Rarely in advanced multiple myeloma, metastatic deposits outside the bone
marrow (extramedullary) are seen.1 Myeloma cells found at
extramedullary site may either be due to extramedullary plasmacytoma (EMP) or
due to extramedullary dissemination of multiple myeloma.6 EMP is
uncommon and is characterised by discrete solitary masses of neoplastic
monoclonal plasma cells outside bone marrow.2 Most common sites for
solitary extramedullary plasmacytoma include mainly upper respiratory tract
such as nasal cavities, paranasal sinuses and nasopharynx without the
involvement of bone marrow.5 Extramedullary dissemination of
multiple myeloma is also uncommon and reported sites include spleen, liver,
lymph nodes, kidney, thyroid gland, adrenals, ovary, testes, lung, pleura,
pericardium, intestinal tract and skin.6 Multiple myeloma
masquerading as pulmonary nodule is extremely rare. Pulmonary involvement in
myeloma is so rare that there is no mention of its occurrence in several large
series. Kintzer et al found that 46% of patients in a series of 958 cases had
thoracic involvement by myeloma. Most of them showed bone involvement or
pulmonary infiltrate secondary to an infectious process. Only 11 patients
developed extramedullary plasmacytoma in the thorax and four patients had
pulmonary infiltrate suggestive of myeloma cell infiltrate (with only one
proven case).7 In another study 19 (4.4%) out of 432 patients of
multiple myeloma were identified as having extramedullary disease, common sites
being lymph node, pleura and soft tissues with only 3 cases (6.2%) occurring
within lung parenchyma.2 Pulmonary involvement seems to be more
commonly associated with aggressive terminal phase of myeloma.3 We
report a case in which pulmonary parenchymal lesion was the initial
presentation of the disease and the diagnosis of multiple myeloma was confirmed
subsequently on investigations.
In diagnostic criteria of multiple myeloma, major
criterias include plasmacytosis on tissue biopsy, bone marrow plasmacytosis
> 30% plasma cells, monoclonal globulin spike on serum electrophoresis (>
3g/dl for IgG, 2 g/dl for IgA) or on urine electrophoresis (>1g/24hr of
kappa or lamda light chain) while minor criterias include bone marrow
plasmacytosis of 10-30% plasma cells, monoclonal globulin spike less than the
level defined above, lytic bone lesions and residual normal IgM<0.05g/dl,
IgA<0.1g/dl, IgG<0.6g/dl. The diagnosis of multiple myeloma requires a
minimum of two major or one major and one minor criteria each or three minor
criteria (always including 1 and 2)
The pulmonary involvement in multiple myeloma needs to
be differentiated from solitary extramedullary pulmonary plasmacytoma, the
treatment and prognosis of the two conditions is vastly different. The
diagnostic criterias for solitary extramedullary pulmonary plasmacytoma are
monoclonal plasma cell histology on tissue biopsy, bone marrow plasma cell
infiltration not exceeding 5% of all nucleated cells, absence of osteolytic
bone lesions or other tissue involvement, absence of hypercalcemia or renal
failure, low serum M protein concentration, if present.9
The most typical thoracic manifestations of multiple
myeloma are bony involvement of thoracic cage or pulmonary infiltrate secondary
to infection. Other described manifestations of myeloma in the lungs include
multiple nodular lesions, diffuse reticulonodular pattern, pulmonary
calcification or amylodosis.2
Multiple myeloma masquerading as pulmonary mass at its
first presentation prompted us to put forward this case report.
REFERENCES
1. Abdalla IA, Tabbara IA. Nonsecretory Multiple Myeloma. South Med J 2002;95(7):56-8.
2. Sullivan PO, Müller NL. Pulmonary and nodal multiple myeloma mimicking lymphoma. BJR
2006; 79: e25-e27.
3. Shin MS, Carcelen MF, Ho
KJ. Diverse roentgenographic manifestations of the rare
pulmonary involvement in myeloma. Chest 1992;102(8);
946-8.
4. Duggal RK, Ramachandran KA. Multiple Myeloma with
Extra-Medullary Dissemination in the Lung. JIACM 2002; 3(1): 93-5.
5. Longo DL, Munshi NC. Plasma cell disorders. In: Fauci et al. Ed.: Harrison’s
Principles of Internal Medicine:17th ed.:
New York: McGraw Hill, 2008; 700-6.
6. Pinto RGW Mandreker S,
Verneker JA. Multiple Myeloma presenting a subcutaneous nodule on the chest
wall: Diagnosis by fine needle aspiration. Acta Cytologica 1997; 41(12):
1233-4.
7. Kintzer JS, Rosenow EC,
Kyle RA. Thoracic and pulmonary abnormalities in multiple myeloma:a review of 958 cases. Arch Intern Med 1978;138(6):727-30
8. Grogan TM, Camp BV, Kyle
RA, Muller HHK, Harris NL. Plasma cell neoplasms. In:
Jaffe ES, Harris NL, Stein H, Vardiman JW. Ed. Pathology and
genetics of tumours of Hemematopoietic and lymphoid tissues. Lyon:2001;142-56.
9. Galieni P, Cavo M, Pulsoni
A, Avvisati G. Clinical outcome of extramedullary plasmacytoma. Haematologica
2000;85(1):47-51.